
Preserve Social Needs Investments Through Strategic Community Health Worker Deployment
By Kamya Sanjay, Associate Director
The landscape for health-related social needs (HRSN) programming has undergone a profound transformation since early 2025. Federal funding cuts, soaring demand for philanthropic dollars, and growing financial pressures on health systems and plans have widened the gap between available resources and the scale of need. Organizations that have long championed HRSN work are being forced to reassess their investments, even as the communities they serve face mounting challenges.
Sustaining meaningful HRSN programs in this environment requires making the case for social needs work to the organizations that stand to benefit from it and building the infrastructure to deliver results they can measure. Community Health Workers, deployed strategically, offer exactly that opportunity. CHWs bring decades of experience bridging healthcare and community, yet their full potential as a sustainable, value-generating workforce remains largely unrealized.
Community Health Workers (CHWs) Meet People Where They Are
CHWs are trusted members of the communities they serve who can effectively bridge gaps between health systems and populations most in need of care. At QV Health Solutions, we've supported several CHW initiatives across a wide range of employment models and care settings.
As the scope of CHW activities spans a broad continuum – from brief, single-touch interventions (e.g., social needs screening and vaccination education) to more intensive, sustained support (e.g., chronic disease management, care transitions from hospital to home, and longitudinal health coaching) – so too does the measurable impact to key healthcare stakeholders.
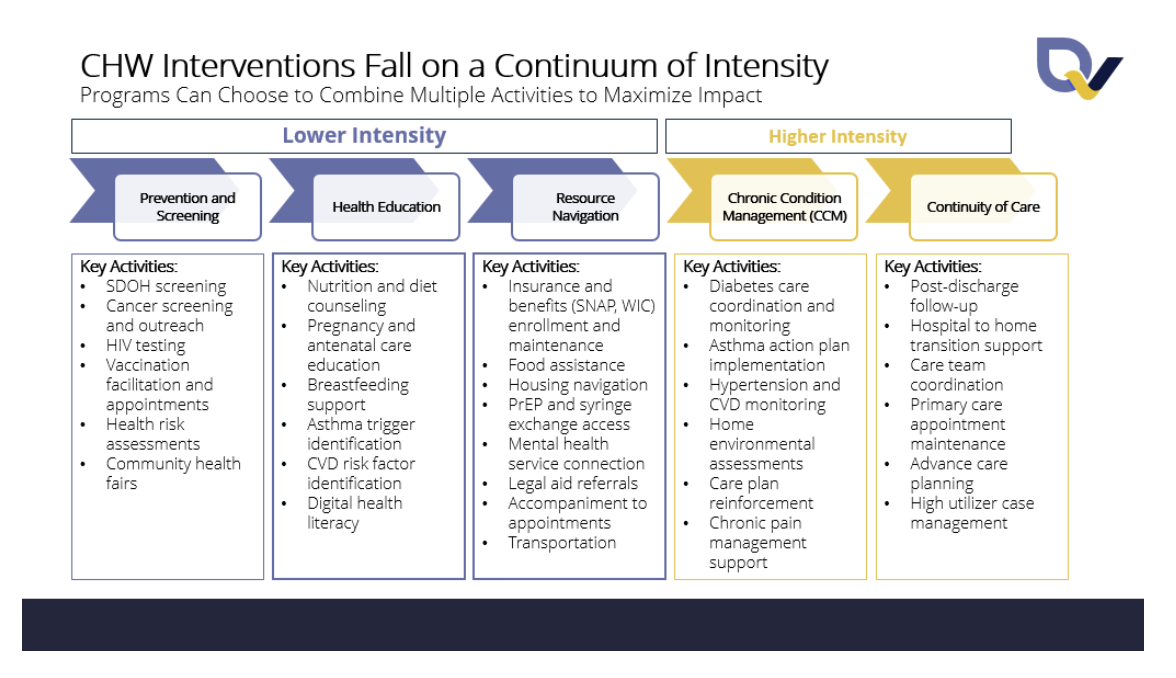
Identifying Impactful CHW Models
A range of factors (e.g., local priorities, payment models) can dictate the shape of CHW engagement. For example, a state Medicaid benefit that compensates CHWs for patient visits but not for community outreach naturally incentivizes models that focus on patients already established within the healthcare system rather than identifying and engaging harder-to-reach individuals.
What distinguishes high-performing CHW programs from those that struggle to demonstrate meaningful impact? Our work with health systems and CBOs suggests several factors that set high-impact programs apart:
Clear role definition. Successful programs clearly delineate between CHW and other professionals like nurses, social workers, and care coordinators. This does not mean they operate in silos; rather, they establish explicit criteria for when patients should be escalated to higher levels of care or coordination, such as nursing or social work. They also avoid the trap of using CHWs as a catch-all role for administrative tasks or unfilled positions.
Top of license deployment. CHWs are most effective when they can operate at the top of their license and engage patients who need their skills most. High-impact programs leverage the uniquely meaningful contributions of CHWs rather than relegating them to tasks that could be performed by administrative staff.
Integration across domains. Strong CHW models create continuity of activities across resource linkage, health promotion, and advocacy rather than single-function siloing. This integrated approach more accurately mirrors patient experience with HSRNs: interconnected across multiple domains of their lives rather than isolated to individual categories.
Measurement and accountability. Programs demonstrating positive outcomes must clearly define models, population served, and results achieved (i.e., meaningful performance metrics). Strong data infrastructure enables ongoing analysis and informs continuous quality improvement; it can also ensure accountability to results and serve as the evidence backbone for sustained funding.
Funding for CHW programs also varies significantly by state. Some states like California, Minnesota, and Oregon provide direct Medicaid reimbursement for CHW services, creating a continuous revenue stream.
However, most programs in states without direct reimbursement pathways must rely on other mechanisms: federal and state grants (many of which are currently constrained), community benefit initiatives, value-based payment arrangements, and private philanthropic investments.
Where to Deploy CHWs for Maximum Impact
While we recognize the broader human and social value of many CHW-led initiatives, this era of more constrained resources calls for consideration of opportunities to deploy CHWs where they can generate the strongest outcomes and most compelling return on investment. The evidence is particularly compelling for the following use cases:
A community health worker provides nutrition education. Licensed under CC BY 4.0.
Outreach to hard-to-reach populations. CHWs excel at engaging individuals not easily reached and/or trusted by traditional healthcare systems (e.g., people experiencing homelessness, immigrants with limited English proficiency, patients with behavioral health needs, or patients living in rural areas with limited transportation).
Associated outcomes: Establish connection to primary care or specialty care, increase preventive care utilization, improve health insurance enrollment.
Support for chronic disease management and care plan adherence. For conditions like diabetes, hypertension, and asthma - where patient behavior and engagement drive outcomes - CHWs add value to clinical care teams. They reinforce treatment plans by teaching patients using culturally resonant and accessible language, providing self-management skills, addressing medication access issues, and helping people overcome practical barriers like transportation and childcare that inhibit adherence to medical advice.
Associated outcomes: Reduce appointment no-show rates, improve care plan adherence, improve chronic health indicators like HbA1c and blood pressure, reduce disease-related emergency department visits.

Community health workers provide guidance during transitions of care and for chronic disease management. Licensed through Shutterstock.
Guidance during transitions of care. Hospital discharge is a high-risk moment of patient vulnerability to readmission and follow-up loss. CHWs who engage patients during or immediately after hospitalization can ensure medications are filled, appointments scheduled and attended, and basic post-discharge needs addressed. The impact case is particularly strong for patients with complex medical needs, lack of family or social support, or limited health literacy.
Associated outcomes: Reduce avoidable emergency department visits, reduce 30-day and 90-day hospital readmissions, improve post-discharge medication adherence, increase primary care follow-up attendance.
Close care gaps in value-based arrangements. For health plans and health systems participating in value-based payment models, closing care gaps directly impacts quality scores and financial performance. CHWs can systematically outreach to patients with care gaps, provide education and coaching, address barriers to care completion, and facilitate appointment scheduling.
Associated outcomes: Improve HEDIS and Star Ratings performance, increase completion of preventive care measures, reduce total cost of care.
Generate revenue through available reimbursement mechanisms. In states with Medicaid CHW reimbursement or for organizations participating in community health initiatives with dedicated CHW funding, deploying CHWs strategically in reimbursable activities can generate revenue that helps sustain the CHW workforce and broader programs supporting HRSNs. This requires more work (i.e., a strategic use of state-specific billing mechanisms and documentation standards) but creates a path toward financial sustainability that is less dependent on time-limited grant funding. Organizations should audit their current CHW activities against reimbursement criteria and adjust workflows to maximize billable services without compromising impact.
Beyond fee-for-service reimbursement, organizations should also explore performance and outcomes-based payment models – such as shared savings arrangements or pay-for-performance contracts tied to utilization reductions or quality improvements – where CHW contributions can be directly attributed to measurable results. These models align financial incentives with the population health goals CHWs are best positioned to advance, and as the evidence base grows, they represent an increasingly viable path to sustainable, scalable CHW financing.
Why Private Organizations Should Consider Funding Community Health Workers
As traditional funding sources contract, some health plans, health systems, and private foundations are evaluating whether to maintain or expand CHW programs through direct investment. But why should private organizations continue to invest in CHWs specifically despite limited resources and competing priorities?
For health plans, health systems, and private foundations, CHWs deliver measurable financial returns alongside better outcomes. Research demonstrates that strong CHW programs return an average of $2.47 per dollar invested to Medicaid payers. The key is ensuring programs are structured to capture and report priority outcomes consistently – such as reduced emergency department utilization, hospital readmission prevention, improved medication adherence, and increased primary care engagement – demonstrating clear attribution between CHW activities and utilization changes.
Health systems benefit through many of the same mechanisms, with each avoided readmission worth thousands of dollars and improved patient satisfaction scores directly impacting reimbursement under value-based programs. CHWs also strengthen connections to primary care, building patient panel size while addressing the social needs that drive avoidable acute care use. For health systems specifically, well-designed CHW programs can also help meet community benefit requirements and quality metrics – adding institutional value beyond direct financial returns.
Private foundations, meanwhile, play a critical role in sustaining and scaling CHW programs that health plans and health systems may not yet fully fund, particularly in communities where the ROI case is still being built. Foundations are also uniquely positioned to pilot new payment models (such as braided funding arrangements, outcomes-based contracts, or CHW integration into value-based care structures) that generate the evidence and infrastructure needed to attract sustainable public and private investment over time.
Beyond financial returns, CHW programs reflect the growing recognition that medical care alone cannot improve health outcomes for populations facing significant social barriers and mistrust of traditional healthcare entities. Organizations that invest strategically in CHWs position themselves to deliver whole-person care that addresses the root causes of poor health.
The Path Forward
While the current funding environment poses increased challenges, it also offers organizations a path toward more intentional articulation of value and deployment of resources to high-impact work.
Organizations looking to sustain or expand CHW programs should focus on three key priorities:
Maximize available reimbursement. Organizations should conduct a comprehensive assessment of available (and potential new) funding mechanisms and then determine the capacity requirements (existing and new) for capturing them. Those operating in states with Medicaid CHW reimbursement can ensure that CHWs are deployed in reimbursable activities and that documentation meets state requirements. This often requires workflow adjustments, staff training on documentation standards, and investment in billing infrastructure; it is critical to assess the extent to which the return justifies the effort. In states without direct CHW reimbursement, CHWs embedded in value-based payment arrangements, Accountable Care Organizations, or hospital community health initiatives may be fundable through those structures.
Demonstrate value to key stakeholders. Developing compelling case studies and return-on-investment analyses strengthens the financial case significantly. Health plans and health systems will invest in CHW programs that deliver measurable and meaningful returns, and address real pain points. This means moving beyond process metrics like "number of screenings completed" and “number of social needs identified” to outcomes like "percentage of high-risk patients connected to primary care" or "reduction in 30-day readmissions."
Deploy CHWs strategically in high-impact use cases. Not every CHW activity generates equal value. Programs that focus CHWs on transitions of care, hard-to-reach populations, care gap closure, and chronic disease support are more likely to demonstrate the impactful outcomes that secure sustainable funding.
CHW programs can become a cornerstone of sustainable HRSN work. Successful programs deploy CHWs where they generate the greatest impact, capture data, and report the outcomes that justify continued investment.
To preserve and advance social needs infrastructure, we must move beyond grant dollars and instead focus on demonstrating the value of HRSN programs to the partners who benefit from the work. This should include efforts to clarify the conditions necessary for achievement of sustained positive impact. Community Health Workers, deployed strategically, offer exactly that opportunity.